
SIBO and Dysbiosis Dynamics: Restoration of Small Intestinal Motility
1. Introduction: The Fermenting Small Bowel
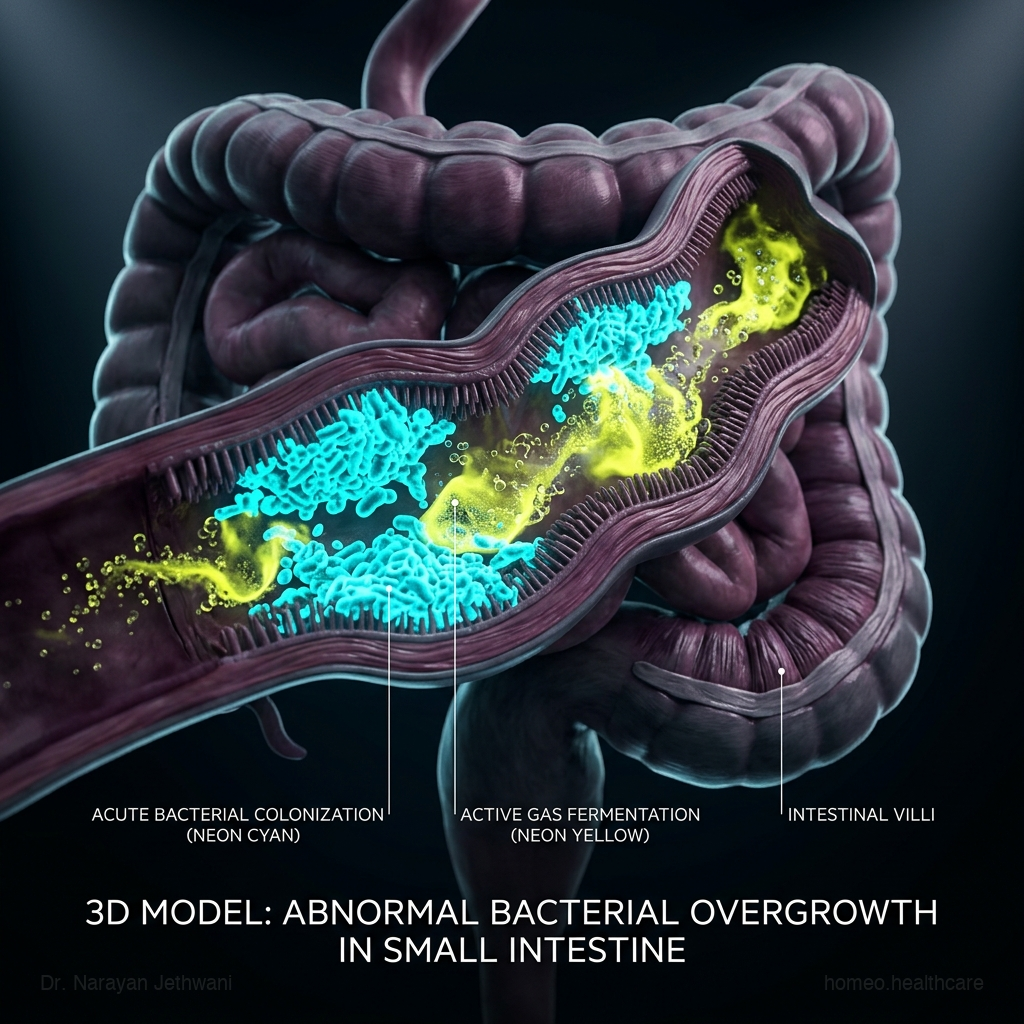
Small Intestinal Bacterial Overgrowth (SIBO) represents a state of severe digestive dysregulation where bacteria normally confined to the large intestine migrate upward and proliferate in high numbers within the small intestine. Unlike the colon, which houses trillions of bacteria, the small intestine should maintain a relatively low bacterial population to prevent interference with nutrient digestion and absorption. When these bacteria accumulate, they ferment incoming dietary carbohydrates, producing large amounts of hydrogen, methane, or hydrogen sulfide gases. This fermentation leads to chronic bloating, abdominal pain, diarrhea, or constipation, and can damage the delicate mucosal lining, resulting in malabsorption and nutritional deficiencies.
At Homeo.Healthcare, we view SIBO not merely as a bacterial infection, but as a functional failure of small intestinal motility. Conventional treatments rely on repeated courses of antibiotics. While this can temporarily clear the bacteria, it does not restore the bowel’s natural clearing wave, leading to recurrence rates as high as 80%. Our constitutional approach aims to restore the Migrating Motor Complex (MMC), improve bile acid synthesis, support mucosal barrier healing, and correct the underlying miasmatic susceptibility. This guide details the pathophysiology of SIBO and outlines the homeopathic pathways to recovery.
2. Physiology of Small Intestinal Motility: The MMC Wave
The primary mechanism preventing bacterial accumulation in the small intestine is the Migrating Motor Complex (MMC). The MMC is a cyclic, wave-like pattern of electrical activity and muscle contraction that sweeps through the stomach and small intestine during periods of fasting (typically every 90 to 120 minutes between meals). The MMC acts as a biological broom, sweeping undigested food particles, cellular debris, and bacteria down into the colon. The MMC is regulated by the enteric nervous system, the vagus nerve, and the hormone motilin, which is released by specialized cells in the duodenum.
The MMC consists of three phases. Phase I is a period of quiescence with little or no contraction. Phase II involves irregular, low-amplitude contractions. Phase III is the active phase, characterized by a short burst of high-amplitude, regular contractions that sweep all luminal contents forward. If the MMC is compromised—often due to chronic stress, thyroid dysfunction, or nerve damage from food poisoning—the clearing wave fails. Food and bacteria remain stagnant in the small intestine, providing a rich substrate for bacterial colonization and fermentation.

3. Pathophysiology: Hydrogen vs. Methane Fermentation and Malabsorption
Bacterial fermentation in the small intestine produces distinct physiological profiles. Hydrogen-dominant SIBO occurs when bacteria (such as E. coli or Klebsiella) ferment carbohydrates, releasing hydrogen gas. This gas stimulates local mucosal secretions and alters motility, presenting with frequent, watery stools and cramping. Methane-dominant SIBO (now classified as Intestinal Methanogen Overgrowth or IMO) arises when archaea (principally Methanobrevibacter smithii) feed on hydrogen gas, producing methane. Methane acts as a paralytic agent on the enteric nervous system, slowing transit time, promoting severe constipation, and worsening gas fermentation.
The chronic fermentation and presence of high bacterial density in the small intestine damage the delicate microvilli, which are responsible for producing digestive enzymes (such as lactase) and absorbing nutrients. The bacteria also deconjugate bile salts, rendering them ineffective for fat digestion. This leads to fat malabsorption (steatorrhea), deficiency in fat-soluble vitamins (A, D, E, K), and the malabsorption of vital nutrients like vitamin B12 and iron, resulting in chronic fatigue, weight loss, and systemic nutrient depletion.
4. Key Clinical Markers and Laboratory Parameters
Accurate diagnosis of SIBO involves measuring bacterial gas production and assessing nutritional markers. The most critical parameters include:
- Lactulose or Glucose Breath Test: Measures exhaled hydrogen and methane gases over a 3-hour period; a rise of hydrogen ≥ 20 ppm or methane ≥ 10 ppm confirms overgrowth.
- Serum Vitamin B12 & Iron: Chronic malabsorption leads to macrocytic anemia (low B12) or microcytic anemia (low iron).
- Stool Elastase: Assesses pancreatic digestive enzyme output, helping to differentiate SIBO from exocrine pancreatic insufficiency.
- HbA1c & Glycemic Markers: Hyperglycemia damages enteric nerves (diabetic autonomic neuropathy), disrupting the MMC wave.
- TSH & Thyroid Panel: Hypothyroidism slows all metabolic processes, directly impairing small intestinal motility.

5. Conventional Treatments and Their Systemic Limitations
Conventional medical management of SIBO relies heavily on non-absorbable antibiotics like rifaximin (sometimes combined with neomycin or metronidazole for methane). While effective at temporarily reducing bacterial populations, antibiotics do not restore the underlying MMC clearing wave. Without restoring motility, recurrence is highly common, leading to repeated courses of antibiotics that can permanently damage the beneficial colonic microbiome. Furthermore, prokinetic medications (such as low-dose erythromycin or prucalopride) are often prescribed to stimulate motility, but these can cause side effects like cardiac arrhythmias, muscle spasms, or lose efficacy over time due to receptor desensitization.

6. The Homeopathic Constitutional & Miasmatic Paradigm
Homeopathy views SIBO not as a bacterial infection to be eradicated, but as a state of functional gut stagnation resulting from an imbalance in the vital force. The constitutional remedy targets the autonomic nervous system, restoring the coordination of the enteric nervous plexuses and stimulating motilin pathways. The miasmatic framework is vital. The Psora miasm drives functional hyper-reactivity, manifesting as rapid gas fermentation, bloating, and spasmodic cramping. The Sycosis miasm governs chronic stagnation, leading to slow transit time, methane-induced constipation, and structural tissue changes. The Syphilis miasm drives destructive tissue patterns, resulting in mucosal degeneration and deep malabsorption. Prescribing anti-miasmatic constitutional remedies helps to restore lasting small intestinal motility and prevent SIBO recurrence.
7. Advanced Homeopathic Materia Medica for SIBO & Motility
The table below details the primary remedies utilized in our clinic to manage SIBO and restore small bowel motility:
| Remedy | Key Modalities & Emotional Profile | Clinical Indications & Tissue Affinity |
|---|---|---|
| Lycopodium Clavatum | Worse from 4 PM to 8 PM, cold drinks, starchy foods; better from warm drinks, passing gas. | Immediate bloating after a few mouthfuls, flatulence, liver congestion, and right-sided abdominal discomfort. |
| Carbo Vegetabilis | Worse from rich food, milk, lying down; better from belching, being fanned. | Severe upper abdominal distension, constant belching that provides temporary relief, complete digestive sluggishness. |
| China Officinalis | Worse from touch, draft of air, fruit; better from hard pressure, double bending. | Bloating of the entire abdomen, passing gas does not relieve discomfort, and severe fatigue due to loss of vital fluids. |
| Plumbum Metallicum | Worse from movement, night; better from hard localized pressure, warmth. | Severe constipation with a sensation of the abdomen being drawn back by a string, dry colonic stools (IMO). |
| Nux Vomica | Worse from stimulants, cold air, anger; better from warmth, resting. | Spasmodic digestive cramps, constipation with ineffectual urging, and toxic overload from antibiotic abuse. |
8. Multi-Dimensional Motility Control
Resolving SIBO requires addressing several physiological and metabolic factors. The bento grid below outlines these core dimensions:
Migrating Motor Complex
Restoring the Phase III clearing wave during fasting prevents bacterial migration and sweeps undigested food particles down into the colon.
Bile Acid Synthesis
Healthy bile flow acts as a natural antimicrobial agent in the small intestine, inhibiting bacterial colonization and supporting lipid digestion.
Enteric Nervous Signaling
Optimizing the coordination between the myenteric and submucosal plexuses ensures smooth, wave-like peristaltic muscle contractions.
Glycemic Autonomic Balance
Preventing chronic high blood sugar protects enteric nerves from diabetic autonomic neuropathy, maintaining natural motility patterns.
9. Clinical Timeline: Restoring Small Bowel Motility
Resolving SIBO and preventing recurrence is a progressive process. The clinical timeline below details our 4-phase protocol:
Reduce abdominal bloating and gas production using targeted remedies (e.g., Carbo Veg or China) to soothe immediate digestive discomfort.
Introduce constitutional remedies (e.g., Lycopodium or Plumbum) to activate the Migrating Motor Complex clearing waves between meals.
Implement a low-fermentation anti-inflammatory diet, support mucosal barrier proteins, and correct fat-soluble vitamin malabsorption.
Maintain healthy motility patterns, optimize thyroid and metabolic health, and perform follow-up breath tests to confirm lasting clearance.
Warning Signs Requiring Urgent Medical Evaluation
SIBO and severe dysbiosis can indicate underlying structural issues. The following symptoms require immediate diagnostic evaluation:
- Fecal Impaction: Severe, persistent constipation with inability to pass gas or stool, accompanied by abdominal vomiting.
- Severe Malabsorption: Rapid weight loss, chronic pale loose stools (steatorrhea), and signs of neurological numbness (due to severe B12 depletion).
- Persistent Fever: Abdominal pain accompanied by fever and chills, suggesting active systemic infection or localized bowel abscess.
10. Frequently Asked Questions (FAQs)
Why does SIBO keep returning after antibiotic treatments?
Antibiotics kill the bacteria but do not restore the small intestine’s physical clearing waves (the MMC). Without these clearing waves, bacteria from the colon migrate back up into the small intestine, leading to rapid recurrence. Homeopathy focuses on restoring MMC function to prevent this recurrence.
Should I take probiotics if I have SIBO?
We generally recommend avoiding high-dose probiotics during the active phase of SIBO, as introducing more bacteria into a congested small intestine can increase gas fermentation. We focus first on restoring motility before reintroducing beneficial strains.
How long does it take to restore normal bowel motility?
While gas and bloating can improve within 4-6 weeks, restoring the coordination of the enteric nervous system and the MMC clearing waves typically requires 3-6 months of consistent constitutional homeopathic care.
Core SIBO Recovery Checklist
- Perform a lactulose breath test to measure hydrogen and methane gas levels.
- Incorporate a low-fermentation diet (e.g., Low-FODMAP) temporarily to reduce gas substrate.
- Ensure at least 3 to 4 hours of complete fasting between meals to allow the MMC clearing wave to execute.
- Optimize thyroid health (TSH levels) to support overall digestive transit speed.
- Schedule a constitutional consultation to identify your customized motility recovery pathway.
Achieving permanent recovery from SIBO requires moving beyond eradication to restore the natural motility of the small intestine. By combining advanced breath analysis with the precision of classical homeopathy, we help you activate the Migrating Motor Complex and restore lasting digestive vitality. Visit our evidence-based medical library to learn more.
Leave a Reply